 Thyroiditis is the medical term used to describe inflammation of the thyroid gland. Most frequently this inflammation of the thyroid gland is the result of Hashimoto’s thyroiditis which is the most common cause of hypothyroidism in the United States. It was named after the doctor who first described the condition in 1912.
Thyroiditis is the medical term used to describe inflammation of the thyroid gland. Most frequently this inflammation of the thyroid gland is the result of Hashimoto’s thyroiditis which is the most common cause of hypothyroidism in the United States. It was named after the doctor who first described the condition in 1912.
This condition is caused by an inflammation of the thyroid gland as the result of an autoimmune attack on the gland. This means that the body’s immune system attacks the thyroid gland, as if it were foreign tissue. The underlying cause of Hashimoto’s thyroiditis continues to be unclear, but researchers do know that it tends to occur in families and is associated with the clustering of other types of conditions such as diabetes and celiac disease.
Hashimoto’s thyroiditis is five to 10 times more common in women than in men. Blood tests reveal an increased number of antibodies to an enzyme found within the thyroid gland. As a result the inflammation develops in the gland and the thyroid is destroyed.
The symptoms of thyroiditis are similar to those of hypothyroidism which are often subtle. This means that they are nonspecific and can mimic the symptoms of many other conditions, some of which are attributed to aging. Individuals who have mild disease may have no signs or symptoms.
Symptoms include fatigue, depression, modest weight gain, cold intolerance, excessive sleepiness, dried coarse hair, constipation, dry skin, muscle cramps, increased cholesterol levels, decreased concentration and vague aches and pains. As the hypothyroidism becomes more severe or, when more of the thyroid gland is destroyed, there may be puffiness around the eyes and a slowing of the heart rate as well as heart failure. In its most profound form, severe hypothyroidism can lead to a life-threatening coma which seems to be triggered by severe illness, surgery, stress or traumatic injury.
A less common form of thyroiditis is De Quervain’s Thyroiditis, also called subacute or granulomatous thyroiditis. This was first described in 1904 and is much less common. In this condition the gland generally swells rapidly and is very painful and tender. It discharges thyroid hormone into the blood and patients immediately become hyperthyroid. Over the next several weeks the hyperthyroidism resolves.
Patients frequently become ill with fever and prefer to stay in bed. Blood work will not reveal thyroid antibodies but the sedimentation rate, which measures inflammation, will be very high. Although it resembles an infection there will be no infectious agents identified and antibiotics are of no use. Nearly all patients will fully recover and the thyroid gland will return to normal after several weeks or months. While recurrences are very uncommon a few patients will become hypothyroid once the inflammation settles down and will need to stay on thyroid hormone replacement indefinitely.
 The third type of thyroiditis is called Silent thyroidits. It is the least common type of thyroiditis and was not recognized until 1970, although it probably existed and was treated as Graves’ disease before that. Silent thyroiditis is a mixture of Hashimoto’s and De Quervain’s thyroiditis. Blood thyroid tests will be high, radioactive iodine uptake will be low and there will be no pain. The results of a needle biopsy will resemble Hashimoto’s thyroiditis.
The third type of thyroiditis is called Silent thyroidits. It is the least common type of thyroiditis and was not recognized until 1970, although it probably existed and was treated as Graves’ disease before that. Silent thyroiditis is a mixture of Hashimoto’s and De Quervain’s thyroiditis. Blood thyroid tests will be high, radioactive iodine uptake will be low and there will be no pain. The results of a needle biopsy will resemble Hashimoto’s thyroiditis.
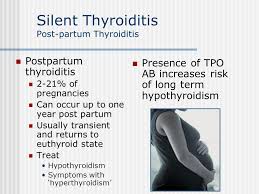
The majority of those affected are young women following pregnancy. The disease usually needs no specific treatment and 80% of those affected will completely recover and return to normal thyroid status after three months. Symptoms will be similar to Graves’ disease, but much milder. The thyroid gland will only slightly enlarge. Treatment will usually be bed rest with beta-blockers to control the palpitations in the heart. Treatments such as radioactive iodine, surgery or anti-thyroid medication, often used for individuals who suffer from Graves’ disease, is never needed. Unfortunately, a few patients will become permanently hypothyroid and require thyroid replacement for the rest of their lives.
The fourth type of thyroiditis is called Reidel’s thyroiditis. This is a very rare form of the disease in which inflammation causes a merging with surrounding structures such as muscle and trachea. Some physicians believe that this is not a form of thyroiditis, but rather a rare form of tumor that happens to involve the thyroid and surrounding tissue.
The thyroid gland itself becomes quite hard and may be very difficult to tell if it’s a result of the inflammation or of cancer. Blood tests are usually normal and a biopsy will be needed to distinguish it from cancer. Since the gland is so difficult to penetrate, a fine needle aspiration may not be possible. Instead, an open biopsy in the operating room may be necessary in order to distinguish this benign disease from a malignant form of cancer. In the most severe form of the disease, the gland becomes so solid it may obstruct the trachea. In this instance an operation will be necessary to remove the middle portion of the thyroid. A complete removal cannot be performed because the thyroid invades normal muscle and other tissue making more extensive surgery very dangerous.
Thyroiditis can also occur in the postpartum period caused by antibodies that attack the thyroid after the delivery of the child. Symptoms will improve within 12 to 18 months but the mother may have permanent hypothyroidism requiring medication. Drug-induced thyroiditis will be caused by prescription drugs such as lithium and cytokines. Symptoms will continue as long as the drug is taken. Radiation-induced thyroiditis follows the treatment with radioactive iodine for hyperthyroidism and certain cancers. Most commonly individuals show symptoms of hypothyroidism which is usually permanent.
Treatment for thyroiditis will depend upon the type of thyroiditis, the extent of the disease, and your overall health. Treatment modalities and recommendations can only be done after your physician has determined the exact thyroiditis that affects you. Once that has been determined, your treatment protocols should be decided by both you and your physician.
Resources:
University of Maryland Medical Center: Thyroiditis
http://www.umm.edu/altmed/articles/thyroiditis-000164.htm
American Family Physician: Thyroiditis: Differential Diagnosis and Management
http://www.aafp.org/afp/2000/0215/p1047.html
Family Doctor: Thyroiditis
http://familydoctor.org/familydoctor/en/diseases-conditions/thyroiditis.html
American Thyroid Association: PostPartum Thyroiditis
http://www.thyroid.org/postpartum-thyroiditis/
US National Library of Medicine: Chronic Thyroiditis
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001409/
Journal of Clinical Pathology: De Quervain’s Subacute Granulomatous Thyroiditis
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC480541/
National Cancer Institute: Thyroid Cancer
http://www.cancer.gov/cancertopics/types/thyroid



Leave a Reply